Photo caption: During the COVID-19 pandemic in Belgium, databases from various sources were linked at the individual level to accurately identify and vaccinate high-priority groups, as well as to monitor vaccination progress and effectiveness.
Photo credit: Sciensano, the National Public Health Institute of Belgium.
How is EUVABECO linking data to optimize vaccination campaigns?
As the COVID-19 pandemic intensified, finding effective vaccination strategies became critical. Successful vaccination campaigns rely on evidence-based approaches and up-to-date data. Collecting new data is time and resource-intensive, so to ease the burden on the healthcare system, Belgium decided to use existing datasets, sparing health workers from additional tasks.
In early 2021, Belgium took an innovative approach by linking databases from various sources at the individual level. Unlike most vaccination campaigns that link data at a coarser level, this approach enabled detailed analysis and personalized insights on exhaustive population data. This allowed Belgium to accurately identify and vaccinate high-priority groups and monitor vaccination progress and effectiveness more effectively.
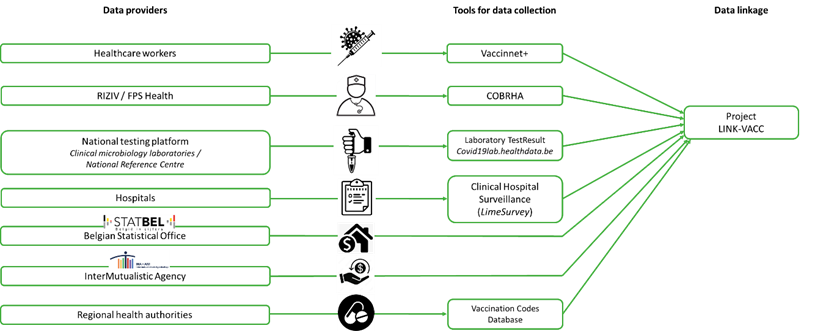
Specifically, Belgium set up the LINK-VACC project. This project linked patient-level data from health registries, testing platforms, and other public and private institutions. It measured vaccine effectiveness against symptomatic infections and hospitalizations and tracked vaccination coverage across different demographic and socio-economic groups. This information is crucial for policymakers to monitor and adjust vaccination campaigns effectively in response to the evolving virus. The LINK-VACC project ensured all data handling was GDPR-compliant, with measures like pseudonymization and secure data storage.
Early in the pandemic, limited vaccine availability made it necessary to prioritize vaccinations for the most vulnerable. In Belgium, medical experts defined priority groups like healthcare workers and the elderly. Using data linkage, these groups were identified based on risk factors like age, health status, and occupation, and invited for vaccination. In addition, non-elderly adults with underlying health conditions, leading to an increased risk of a severe COVID-19 infection, were prioritized as well. Around 1.5 million out of 7 million persons aged 18-64 years were identified as high-priority within this category using data from insurance records, general practitioners, and other healthcare sources.
Building on this model, EUVABECO’s partner Sciensano, the National Public Health Institute of Belgium, is collaborating with other EUVABECO partners in Luxembourg (Agence eSanté Luxembourg), Poland (Wroclaw Medical University), Greece (University of Crete), and Portugal (General Health Directorate) to adapt and apply the model to other national surveillance systems.
Each of EUVABECO’s partner countries has unique healthcare infrastructures and needs, leading to variations in their implementation strategies. Access to accurate, real-time data is essential to address specific public health questions and develop effective policies. In preparation for pilot implementation in September 2024, each country is currently defining objectives and data requirements while organizing data flows to ensure the strategies are relevant and functional in their contexts.
EUVABECO aims to create adaptable and sustainable data linkage plans beyond the pilot phases, targeting broad adoption across all EU Member States. This involves creating detailed work plans, policy recommendations, outbreak response strategies, and criteria for evaluating the system’s impact, as well as considering financial strategies for widespread implementation. These validated plans will be publically released as part of the EUVABECO implementation packages in 2026.
Want to know more?
For more information about EUVABECO, please contact us directly at .